Hepatitis C virus (HCV) is small, enveloped positive-sense single stranded RNA containing virus of a family flaviridae. Viral genome consists of 9,600 bp and is divided into 10 different genes. It is a major public health concern worldwide.

HCV is a major causative agent for chronic hepatitis and also causes hepatocellular carcinoma. It is a small hepatotropic virus infecting 200 million people globally. The World Health Organization (WHO) report states that 3% of the world population is infected with HCV, and every year, 3–4 million new cases of HCV infection occur globally.
In Pakistan, around 11 million people are suffering from HCV, with a very high mortality and morbidity rate The viral RNA is translated into a single polyprotein, which is then cleaved into individual protein by the action of viral and host peptides. The polyprotein is co- and post-transnationally processed by viral and cellular proteases to produce four structural (Core, E1, E2 and P7) and six non-structural (NS2, NS3, NS4A, NS4B, NS5A, and NS5B) proteins.
HCV seroprevalence in Pakistan
Pakistan ranked second in the world in terms of HCV burden, HCV cause 11 million infections all over the Pakistan. Due to poor socioeconomic situation and lack of awareness in different parts of Pakistan this viral infection is increasing day by day. The major HCV infections routes include unsafe dental and general surgery procedures, unsafe blood transfusion, re-use of syringes, unsafe barbers’ tools/beauty salon equipment/ear-nose piercing guns, and so on.
Above all, unawareness among the infected and general population about the transmission routes is further escalating the viral burden in the society. Being a cirrhotic state, the information about the prevalence of HCV in the general population is very less and is confined to urban areas only. A comprehensive review of previous data (2010–2016) about HCV prevalence in the general population showed that the prevalence of HCV in the general population ranged from 3.13% to 23.83%.
The investigated high-risk groups include hepatocellular carcinoma, pregnant women, multi-transfused population, prisoners, homosexual community, urological patients, surgery patients, type II diabetes patients, intravenous drug users, healthcare workers, and end-stage renal disease. The prevalence range of HCV in these high-risk groups ranged from 2.9% to 66%.
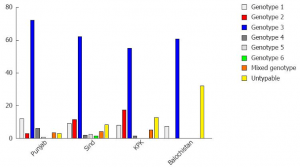
HCV polymerase (NS5B) is error prone and due to the error-prone nature of viral polymerase, HCV has many genotypes and subtypes. Viral genotyping is done from 5¢UTR, core and NS5B region of the genome. Determination of the viral genotype is important for the proper management of the disease, as the antiviral therapy is genotype specific. The interferon-based and direct acting antivirals (DAAs) response is genotype dependent, and different viral genotypes showed a different sustained virological response (SVR).
Treatment
The main purpose of chronic HCV treatment is to achieve high SVR rate and to avoid the development of liver-related complications. Previously, interferon plus ribavirin-based antiviral therapy played an important role in HCV management across the world and showed about 50–80% SVR in patients infected with HCV GT-1/GT-4 or HCV GT-2/ GT-3, respectively.
The response can vary according to the interleukin-28B (IL-28B) genotype. With the advancements of DAAs development, a combination of interferon/ ribavirin and DAAs resulted in about 90% SVR in IL-28B favourable genetic makeup and also shortened the therapy duration. But interferon-based antivirals have many side effects and have resulted in discontinuation of therapy in a large number of individuals.
Direct acting antivirals (DAA) are very costly and that only sovaldi is available in Pakistan on discounted rate Sovaldi (Sofosobuvir, NS5B inhibitor) will be the future treatment drug for Pakistan. Sovaldi showed promising results against GT-3/GT-2 and also is a part of the interferon-free regimen against GT-1. However, in the near future, interferon-based regimens will also be in use because of the unavailability of other DAAs (except Sovaldi)
Conclusion
Pakistan is a developing country with a low socioeconomic status. The government’s health budget is very low in comparison with population needs. In such circumstances with almost no existence of a proper health insurance system across the country, it is very difficult to treat 11 million individuals. Currently, patients are being treated with interferon based antiviral regimen, which showed quite good results, as the major prevalent HCV genotype is (GT-3) interferon sensitive.
Many drawbacks of the treatment are also reported, such as side effects of therapy, relapse cases, emergence of treatment resistance, and increasing number of cirrhosis cases. Moreover, a large proportion of infected individuals were not able to be treated by this regimen. Recently, Sovaldi is approved for treatment. Interferon-based antiviral regimens will also be in use for the future, as they showed good SVR against favourable (GT-3) genotype. To achieve higher SVR against GT-1 and avoid side effects due to interferon-based regimens, there is an urgent need for approval of other DAAs such as Ledipasvir, on discounted price.